Socket Designs and Casting Techniques
Part One | Part Two | Part Three | Part Four | Part Five | Part Six | References
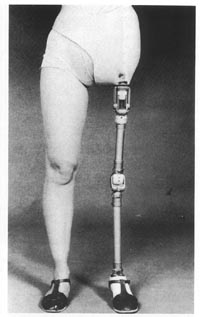 |
FIG21B-9
|
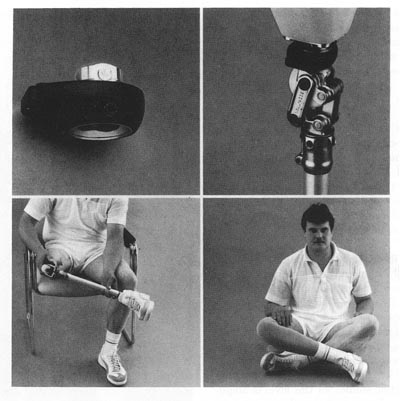 |
FIG21B-10 The transverse rotation unit can be unlocked to permit passive rotation of the shank. This facilitates entering and exiting automobiles, restaurant booths, and simular confined spaces as well as sitting cross-legged on the floor. (Courtesy of Otto Bock Industries, Minneapolis.) |
The most important part of any prosthesis is the socket, which provides the man-machine interface.During the initial assessment of the amputee, examination of postoperative radiographs and careful palpation of the pelvis are recommended. Some amputees present as "hip disarticulation" when they have a short femoral segment remaining or as "transpelvic" when part of the ilium, sacrum, or ischium remains. Unanticipated bony remnants can become a puzzling source of discomfort. On the other hand, they may sometimes be utilized to assist suspension or rotary control or to provide partial weight-bearing surfaces.
Due to the success of ischial containment transfemoral sockets, the importance of precise contours at the ischium and ascending ramus is now more widely recognized.56 The same principles can readily be applied to hip disarticulation sockets to increase both comfort and control57 (Fig21B-11). We prefer to have the amputee simulate weight bearing during the plaster impression technique to create as precise a mold as possible. However, in contrast to the technique advocated by Otto Bock, we believe that careful attention to shaping the medial wall in the ischial region is important to improve control of the prosthesis for both walking and sitting. A sling suspension system should be utilized, in addition, to firm up redundant soft tissue for obese individuals or transpelvic amputees.16,17 (A casting platform alone will suffice for many hip disarticulates, especially those of slight build.)
Soft rubber tubing or a similar shaping device can be pulled snugly about the waist just proximal to the iliac crests to ensure good definition of this critical suspension area and simultaneously define the contours of the thoracolumbar region (Fig21B-12).
If the distance from the iliac crest to the ischial tuberosity is too large in the mold, the socket will piston up and down with every step. Prior to the removal of the plaster mold, the ischial tuberosity area may be highlighted by adding more plaster splints while cupping the ischium firmly in the palm of the hand. The goal of casting is to create an exact replica of the pelvis including the often neglected areas inferior to the lateral, anterior, and posterior aspects of the iliac crest. During model rectification, relief must be provided for the inferior pubic ramus and public tubercle as well as the proximal edge of the iliac crests.
The transpelvic socket requires careful attention to the distal contours for proper weight bearing. In addition to using the sling casting technique to firm the tissues, it is useful to contour the area of the contralateral gluteal fold precisely. Although this can be done by hand, a racingstyle bicycle seat makes a useful adjunct when casting (Fig21B-13).
This contour may add a measure of gluteal bearing on the contralateral side. More importantly, it prevents the hemipelvis from slipping through the inferior border of the socket and adds significant weight-bearing stability. Good distal contours often provide sufficient weight-bearing stability to allow the proximal border of the socket to be trimmed far below the second rib margin, which was considered the proper trim line 30 years ago16,17,26,39.
It is rarely necessary to extend the socket onto the thorax if the distal contours are correct. In like manner, the anterodistal trim line should be as close to the midline as tolerable lest the panniculus protrude hernia-like during weight bearing. The male genitalia should be placed to the side prior to casting to permit the smallest practical anterodistal opening for the transpelvic socket. Although firm oblique counterpressure toward the midline does reduce perineal shearing forces, as noted by Lyquist,36 it should not be overdone. Gentle contouring with the palm of the hand, combined with the sling suspension provides sufficient compression. Many materials are suitable for socket fabrication. As is the case with other levels of lower-limb amputation, the most commonly utilized socket material is a rigid thermosetting resin: polyester or acrylic.47,50
An increasing trend toward more flexible thermoplastic materials is evident, as in other aspects of prosthetic practice.22,38 One of the authors (J.W.M.) has fitted more than two dozen polypropylene/polyethylene copolymer sockets for hip-level amputation over the past decade with good longterm results in durability, comfort, and patient acceptance (Fig21B-14). The recent advent of laminating silicone rubbers allows even more flexibility than do available thermoplastics. As was noted earlier, the resulting comfort and range of motion has been associated with significantly higher rates of prosthetic usage. Although the fabrication is complex, difficult and the finished result slightly heavier than thermoplastic designs, favorable patient response and good durability recommend further development and more widespread application of this technique. The senior author (T.v.d.W.) has fitted 35 silicone rubber sockets over the past 2 years. Amputees who have previously worn more rigid designs typically describe the rubberized sockets as feeling "more natural" or "more like a part of me" (Fig21B-15).
We have divided this article up into sections for faster load times as follows:
Part One | Part Two | Part Three | Part Four | Part Five | Part Six | References