Foot Mechanisms
Part One | Part Two | Part Three | Part Four | Part Five | Part Six | References
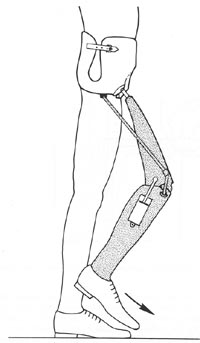 |
FIG21B-7 |
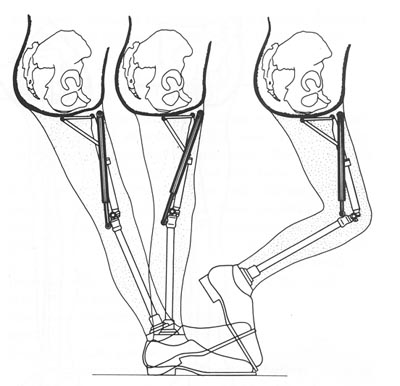 |
FIG21B-8
Modified Hydrapneumatic knee mechanism to provide smooth, coordinated hip and knee motion, as advocated by Lehneis et al. (From Lehneis HR, et al: Prosthetics Management for High Level Lower Limb Amputees. New York Institute of Rehabilitation Medicine, 1990. Used by permission.)
|
Traditionally, the solid-ankle cushionheel (SACH) foot has been recommended for the Canadian hip disarticulation design due to its moderate weight, low cost and excellent durability.16,42 So long as the heel durometer is very soft, knee stability with this foot has generally been quite acceptable. In those cases where slightly more knee stability is desired, a singleaxis foot with a very soft plantar flexion bumper is preferred. Added weight, maintenance, and cost plus reduced cosmesis are the liabilities of this component.46 Multiaxis feet (such as the Greissinger) have liabilities similar to the singleaxis versions but add extra degrees of freedom in hindfoot inversion/eversion and transverse rotation. In addition to accommodating uneven ground, absorbing some of the torque of walking, and-protecting the patient's skin from sheer stresses, multiaxis feet seem to decrease the wear on the other prosthetic mechanisms as well. In the last 5 years, more sophisticated foot mechanisms have reached the market, and all have been demonstrated to function successfully for the high level amputee. The solid-ankle flexible-endoskeleton (SAFE) foot inaugurated a class that could be termed "flexible-keel" designs.45
Other members of this class include the STEN foot and the Otto Bock Dynamic foot. All are characterized by a softer, more flexible forefoot that results in a smoother rollover for the patient. The SAFE version offers some transverse rotation as well.3 In general, a softer forefoot requires special care during dynamic alignment to ensure that knee buckle does not occur inadvertently. However, when used in concert with a polycentric knee, the reverse occurs: the prosthesis actually becomes more stable during late stance phase.
The polycentric knee mechanism strongly resists a bending moment, which leads to its powerful stability at heel strike. It flexes during swing phase only if the forefoot remains firmly planted on the floor as the body "rides" the prosthesis over it.48 This creates a shearing force that disrupts the linkage and permits easy flexion of the knee. Because the softer flexible keel delays this shearing moment, the polycentric knee is actually more stable in late stance than with a more rigid foot.
Dynamicresponse feet, which provide a subjective sense of active pushoff, can also be used to advantage for the hiplevel amputee. The Carbon Copy II, Seattle foot, Springlite, and FlexFoot have all been success fully utilized for this type of patient. They seem to provide a more rapid cadence, as noted by one longterm hip disarticulation wearer, who stated after receiving a Seattle foot, For the first time in my life I can pass someone in a crowd."45 Once again, the interaction between the foot and knee must be carefully monitored. In general, the more responsive the foot mechanism, the more important the knee unit resistances become. Many clinicians prefer fluid-controlled knees, or at least one with powerful friction cells. Otherwise, much of the forward momentum of the shank can be wasted as abrupt terminal impact of the knee. Presumed reductions in energy consumption with the newer feet have not yet been documented by scientific studies for this level of amputation but have been demonstrated under certain circumstances for transtibial amputees. In addition to foot mechanisms, several ankle components have recently reached the American market. These can be paired with most of the feet mentioned above to add additional degrees of motion as desired. Examples include the SwePro ankle from Sweden,
The Blatchford (Endolite) MultiFlex ankle from England, and the Seattle ankle. Torque-absorbing devices are often added to hip disarticulation/transpelvic prostheses to reduce the shear forces transmitted to the patient and components. Ideally, they are located just beneath the knee mechanism (Fig21B-9). This increases durability by placing the torque unit away from the sagittal stresses of the ankle while avoiding the risk of introducing swing-phase whips (which can occur if it is placed proximal to the knee axis). The major justification for such a component is that the highlevel amputee has lost all physiologic joints and, hence, has no way to compensate for the normal rotation of ambulation.52
Finally, transverse-rotation units or positional rotators originally developed for the Oriental world have become available worldwide. Installed above the knee mechanism, these devices permit the amputee to press a button and passively rotate the shank 90 degrees or more for sitting comfort (Fig21B-10). They not only facilitate sitting cross-legged upon the floor but also permit much easier entry into restaurant booths and other confined areas. This component is particularly advantageous for entering and exiting automobiles.
We have divided this article up into sections for faster load times as follows: