Suction Suspension
Part One | Part Two | Part Three | Part Four | Part Five | Part Six | References
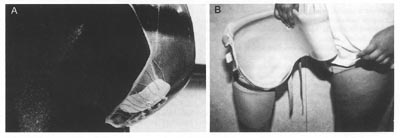
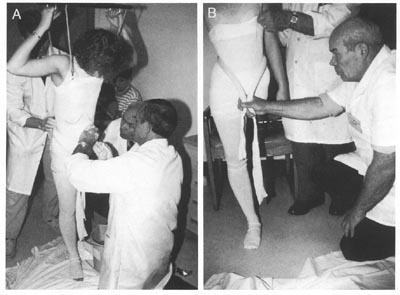
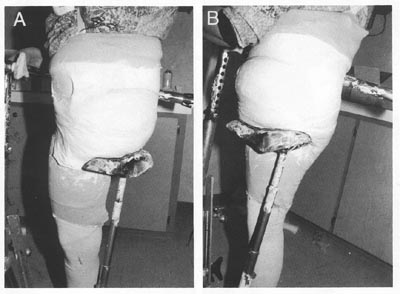
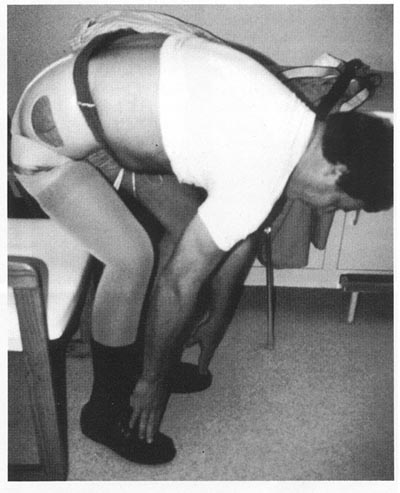
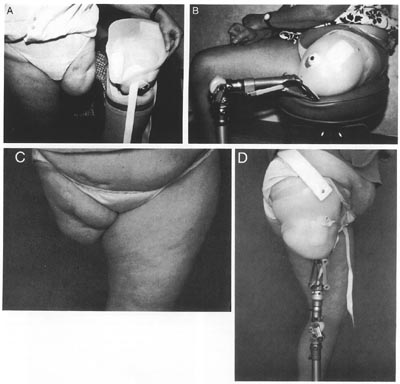
Nearly 40 years ago, Hutter reported a single case of successful fitting of a transfemoral suction socket to a hip disarticulate with a mass of redundant tissue distal to the ischium. The senior author (T.v.d.W.) has personally fitted three such cases recently.
Each was able to ambulate successfully and to retain full suction suspension with only the assistance of a thin, elastic Silesian belt despite the total absence of any femur. The major difference in socket configuration is the creation of a trough like channel to contain both the medial and lateral aspects of the ischiopubic ramus since no femur remains. Such fittings have been done on an experimental basis where there is sufficient residual muscle tissue to create both suction suspension and biomechanical "locking" to stabilie the socket on the patient. This approach warrants further followup and evaluation to determine its practicality.
 |
|
 |
|
 |
|
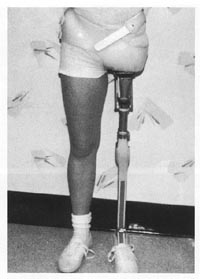 |
FIG21B-14 |
 |
|
 |
Conclusions
Although wearing a transpelvic or hip disarticulation prosthesis may be cumbersome, when fitted within a few weeks of amputation, the initial acceptance rate appears to be similar to that for transfemoral amputation. Immediate postoperative fitting is technically feasible but rarely performed today. Long term wearing rates increase significantly when sockets are comfortable, flexible, and carefully aligned. In view of the magnitude of loss at this level, application of newer, sophisticated joint and foot mechanisms is often helpful. Every case requires review on its own merits; careful attention to socket design, components, and alignment ultimately determines the effectiveness of the prosthesis.
We have divided this article up into sections for faster load times as follows: